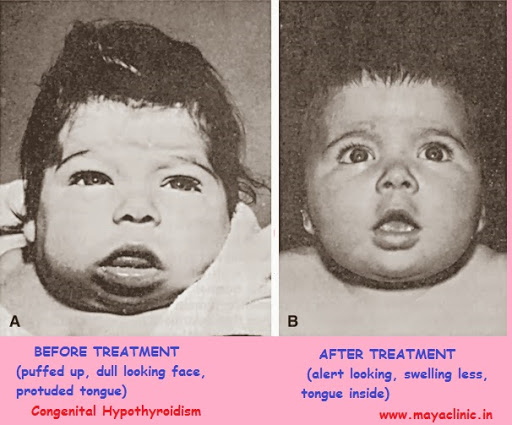
Few months back, I took a Stanford CME Course on an endocrine disorder called congenital hypothyroidism. CH is a condition, present at birth, dealing with an impaired thyroid gland. The disease is fairly common, estimated to occur once in every two thousand five hundred infants. It is extremely important that the diagnosis and treatment occur rapidly because the brain desperately needs thyroid hormones as they are crucial to development. Prognosis gets significantly worse if the disease is not treated in time – if the treatment is started within three months, the mean IQ is 71, but if it is started within six months, the mean IQ is 54. Many times the baby is asymptomatic for the first 6-12 weeks, so it is extremely important to screen for the disease early on to prevent mental retardation.
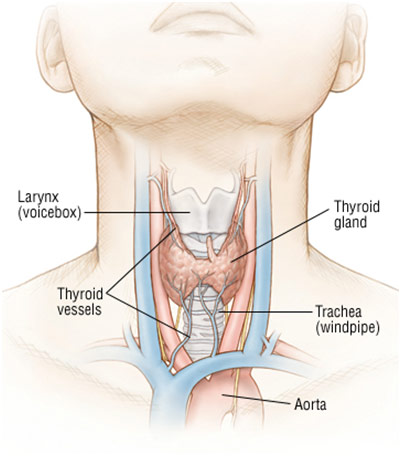
Location of the Thyroid Gland in the Human Body
The thyroid gland is influenced by hormones from the hypothalamus and pituitary, which regulate the other glands. The hypothalamus secretes TRH (thyrotropin-releasing hormone), which stimulates the pituitary to release TSH (thyroid-stimulating hormone). TSH makes the thyroid gland produce T3 (triiodothyronine) and T4 (thyroxine). If T3 and T4 levels get too high, the hypothalamus will process the information and stop the pituitary from making TSH. Similarly, if T3 and T4 levels get too low, the hypothalamus will sense this and make the pituitary release more TSH. In a person with congenital hypothyroidism, there will be low T3 and T4 levels but elevated levels of TSH. The hypothalamus and pituitary are doing their job, trying to stimulate the thyroid; however, the thyroid doesn’t recognize these signals. Thus, the thyroid is underactive because overall T3 and T4 levels remain low. Because the thyroid regulates metabolism and growth, some symptoms of congenital hypothyroidism are umbilical hernia (intestine pushes through the belly button in the abdomen), hypotonia (reduced muscle tension), macroglossia (swollen tongue), bradycardia (slow heart rate), lethargy, and growth failure.
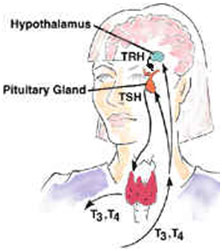
Negative Feedback Loop of TRH, TSH, T3/T4
Congenital Hypothyroidism mostly is present when there is underdevelopment (hypoplasia) or inadequate function of the thyroid gland (aplasia). Eighty-five percent of the time it is due to an anatomical problem with the thyroid gland. For example, the thyroid gland may fail to migrate to the correct position in the neck, making it ectopic. Fifteen percent of the time, however, there is a defect of one of the enzymes needed to make the thyroid hormone. This genetic trait is recessive, so there is a twenty-five percent chance of the subsequent child getting it if both parents carry the gene. It is extremely important to screen for hypothyroidism and initiate treatment early to ensure the best prognosis. In most states, screening for CH is mandatory. If the lab test comes back with TSH levels greater than forty microunits per milliliter, then one can confirm a diagnosis of CH. The most common treatment is in form of Levothyroxine tablets, and the dosage is based on the infant’s weight.
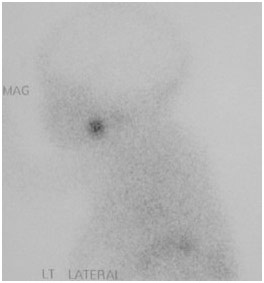
Tc-Pertechnetate Scan of an Ectopic Thyroid Tissue (located at base of tongue instead of neck)
While Congenital Hypothyroidism is a lifelong disease, with proper care, it is entirely possible for one to live an entirely normal life. Nevertheless, it is important to continue treatment and not become careless about taking the medication. While there is no cure at the moment for CH, someday in the future it may be possible to cure the disease so that the thyroid can produce T4 and T3 on its own, taking away the need for medications.
REFERENCES
Before and After Treatment. Maya Clinic, mayaclinic.in/patient-education/category/genetic-metabloic-disorder/. Accessed 19 June 2017.
“Congenital Hypothyroidism.” Genetics Home Reference, National Institutes of Health, ghr.nlm.nih.gov/condition/congenital-hypothyroidism#definition. Accessed 19 June 2017.
“Congenital Hypothyroidism: What Every Primary Care Provider Needs to Know.” Stanford Center for Continuing Medical Education, Stanford Medicine, med.stanford.edu/cme/courses/online/hypothyroidism.html. Accessed 19 June 2017.
Daniel, Maala S. “Congenital Hypothyroidism.” Edited by Stephen Kemp. Medscape, WebMD, 16 Dec. 2015, emedicine.medscape.com/article/919758-overview. Accessed 19 June 2017.
Lee, Kimberly G. “Neonatal Hypothyroidism.” MedlinePlus, 27 Apr. 2015, medlineplus.gov/ency/article/001193.htm. Accessed 19 June 2017.
Sargis, Robert M. “How Your Thyoid Works: Controlling Hormones Essential to Your Metabolism.” Endocrineweb, Vertical Health, www.endocrineweb.com/conditions/thyroid/how-your-thyroid-works. Accessed 19 June 2017.
Thyroid Gland. Drugs, www.drugs.com/health-guide/hypothyroidism.html. Accessed 19 June 2017.













{kind=link}